On October 9, 2024, the Union Cabinet approved extending the free fortified rice supply under welfare programs until December 2028.
Why Rice Fortification is needed?
Widespread Micronutrient Deficiency: India faces a significant public health challenge with micronutrient deficiencies, particularly iron, Vitamin B12, and folic acid. Anaemia, caused by iron deficiency, is a persistent issue affecting large segments of the population, including children, women, and men.
Rice as a Staple Food: Given that 65% of India’s population consumes rice as a staple, it is an ideal vehicle to deliver essential micronutrients to combat these deficiencies, helping improve overall health, productivity, and cognitive development.
Process of Rice Fortification:
Fortified Rice Kernels (FRK): The process involves producing fortified rice kernels that are enriched with essential micronutrients such as Iron, Folic Acid, and Vitamin B12.
Blending with Regular Rice: These fortified kernels are then blended with regular rice at a ratio prescribed by FSSAI (Food Safety and Standards Authority of India).
Typically, fortified kernels make up 1-2% of the total rice, ensuring consistent delivery of micronutrients without altering the taste or cooking properties of the rice.
How the Fortification Initiative has fared so far?
The rice fortification scheme was implemented in three phases between 2022 and March 2024, with the target of achieving universal coverage in all government schemes by March 2024 successfully met.
Fortified rice is now supplied under major welfare programs like the Targeted Public Distribution System (TPDS), Integrated Child Development Service (ICDS), and PM POSHAN in all states and Union Territories.
The initiative is fully funded by the central government, highlighting its commitment to tackling malnutrition and ensuring inclusive nutritional security across the country.
How can food fortification help reduce malnutrition in India?
Combats Micronutrient Deficiencies: Fortifying staple foods with essential nutrients like iron and vitamins helps reduce widespread deficiencies that cause anemia and poor health.
Wide Reach: Through existing public programs (PDS, ICDS), fortified food reaches vulnerable populations, ensuring consistent nutrient intake for large segments of society.
Cost-Effective: It offers a scalable, affordable solution to malnutrition, improving health outcomes without significant changes in diets or eating habits.
Way forward:
Strengthen Monitoring and Quality Control: Implement robust monitoring mechanisms to ensure the consistent quality of fortified rice and its proper distribution across welfare programs to maximize nutritional benefits.
Raise Awareness and Promote Consumption: Conduct awareness campaigns to educate the public on the health benefits of fortified rice, ensuring higher acceptance and consistent consumption to address widespread micronutrient deficiencies.
Four years after the onset of Covid, an expert group formed by NITI Aayog has proposed the establishment of a comprehensive framework to handle future public health emergencies or pandemics effectively.
Lessons Learned from COVID-19:
Gaps in Legal Frameworks: Existing laws like the Epidemic Diseases Act (1897) and National Disaster Management Act (2005) were insufficient for handling large-scale health emergencies. These laws lack clarity on definitions of epidemics and provisions for managing public health crises, drug distribution, and quarantine measures.
Delayed Response and Coordination: The COVID-19 pandemic exposed weaknesses in coordination between central and state governments, highlighting the need for a more organized response mechanism.
Inadequate Surveillance: Insufficient disease surveillance and early warning systems delayed the identification of threats. The role of zoonotic diseases, especially viruses linked to bat species, underscored the need for better monitoring of human-animal interactions.
What specific recommendations does the NITI Aayog report make?
Enactment of PHEMA: Introduce the Public Health Emergency Management Act for a more robust legal framework to manage pandemics and other health emergencies.
Empowered Group of Secretaries (EGoS): Establish a central committee to oversee pandemic preparedness, governance, R&D, surveillance, and response efforts.
Strengthened Disease Surveillance: Create a national biosecurity and biosafety network and monitor human-animal interfaces, especially for zoonotic diseases.
Emergency Vaccine Bank: Develop a stockpile of vaccines for rapid access during health crises, sourced domestically or internationally.
Early Warning and Research Network: Build a forecasting and modelling network, along with Centres of Excellence (CoEs) to advance research on priority pathogens and preparedness.
How can India enhance its pandemic preparedness framework? (Way forward)
Strengthening Legal and Institutional Frameworks: Enact a Public Health Emergency Management Act (PHEMA) and establish an Empowered Group of Secretaries for coordinated pandemic response.
Enhancing Surveillance and Early Warning Systems: Build a robust disease surveillance network, biosecurity system, and epidemiology forecasting for early detection and response to outbreaks.
Investing in Health Infrastructure and Vaccine Stockpiles: Develop public health cadres, boost healthcare infrastructure, and create an emergency vaccine bank for rapid deployment during health crises.
The “Arogya Sanjeevani Policy” serves as a reference point for choosing health insurance for hospitalisation.
AboutArogya Sanjeevani Policy:
Details
Launch Date
April 2020
Issued by
Insurance Regulatory and Development Authority of India (IRDAI)
Objective
To provide basic and affordable health insurance coverage to all citizens
Sum Insured
₹1 lakh to ₹5 lakh per policy year
Coverage
Hospitalization, pre and post-hospitalization expenses, daycare procedures, AYUSH treatments, COVID-19 coverage
Pre-Existing Conditions
Coverage after 4 years of continuous policy renewal
Co-Payment
5% co-payment on all claims
Premium
Varies based on age, sum insured, and insurer
Waiting Period
30 days for new policies; 48 months for pre-existing diseases
Daycare Procedures
Covers over 50+ daycare treatments
Room Rent Limit
Up to 2% of the sum insured per day (maximum ₹5,000 per day)
ICU Room Rent
Up to 5% of the sum insured per day (maximum ₹10,000 per day)
AYUSH Treatments
Covers Ayurveda, Yoga, Naturopathy, Unani, Siddha, and Homeopathy treatments
Maternity Coverage
Not covered
Network Hospitals
Cashless facility in network hospitals
Eligibility
Individuals aged 18 to 65 years
PYQ:
[2019] Performance of welfare schemes that are implemented for vulnerable sections is not so effective due to the absence of their awareness and active involvement at all stages of the policy process – Discuss.
Primary care remains underdeveloped, while the private sector has seen significant growth in secondary and tertiary care.
What are the major necessities in Public Health?
Diseases of Poverty: This includes health issues predominantly affecting the poor and vulnerable populations, such as tuberculosis, malaria, undernutrition, maternal mortality, and illnesses caused by food and water-borne infections like typhoid and diarrheal diseases.
Addressing these needs is critical not only from a health perspective but also as a matter of human rights.
Middle-Class Health Concerns: The second category focuses on health issues related to environmental pollution, including air and water quality, waste management, and food safety.
These issues are often exacerbated by inadequate infrastructure and poor market regulations, leading to chronic illnesses and road traffic accidents.
Curative Care Needs: The most visible public health needs are those related to curative care, which is divided into three levels: primary, secondary, and tertiary care.
The poor often rely on public primary health care for affordable services, while secondary care remains historically neglected.
Tertiary care is primarily addressed through government schemes like the Pradhan Mantri Jan Arogya Yojana (PMJAY) under Ayushman Bharat, aimed at providing coverage for serious health issues.
How do the private hospitals become a real beneficiary in present times?
Limited Coverage: India’s health insurance primarily covers only hospitalisation expenses, leaving out outpatient and primary care services. This benefits private hospitals as they can monopolise high-cost medical treatments, while the larger uninsured population faces commercialised care at market rates.
Weakening of Public Health Sector: The government’s shift in focus from strengthening public sector health care to outsourcing via insurance schemes like PMJAYindicates a failure to build adequate secondary and tertiary public health services.
Threats to Public Healthcare:
Neglect of Secondary and Tertiary Care: The inadequate investment in strengthening secondary- and tertiary-level health care in the public sector, leads to a reliance on private hospitals.
Transformation of Primary Health Centres (PHCs) and Sub-centres: The conversion of sub-centres and PHCs into Health and Wellness Centres (HWCs) has undermined their original role in preventive and promotive health care.
Loss of Trust in Public Healthcare: Due to overcrowding, poor infrastructure, and inadequate funding, public health institutions are losing credibility. Coupled with the commercial interests of private providers, this creates a dual crisis of access and quality in the healthcare system.
Rebranding of Health Centres: The recent renaming of HWCs as “Ayushman Arogya Mandirs” raises concerns about cultural relevance and secularism in public health institutions, especially for non-Hindi-speaking populations, further undermining trust in the system.
Way forward:
Strengthen Public Healthcare Infrastructure: Invest in enhancing secondary and tertiary care facilities in the public sector to reduce dependence on private hospitals.
Integrate Health Insurance and Primary Care: Expand health insurance coverage to include outpatient and primary care services, and ensure that public health centers retain their focus on preventive and promotive care.
Mains PYQ:
Q Public health system has limitation in providing universal health coverage. Do you think that private sector can help in bridging the gap? What other viable alternatives do you suggest? (UPSC IAS/2015)
The recent brutal rape and murder case in Kolkata has sparked widespread calls for the death penalty for the accused.
The Justice J.S. Verma Committee, formed in response to the 2012 Delhi gang rape, recommended against the death penalty for rape, even in the rarest of rare cases, arguing that it would be a regressive step.
Deeper problem in the Health Care Sector:
Healthcare Violence: The protests by resident doctors stem from a series of violent attacks against medical personnel. This violence often arises from disgruntled patients and their families who perceive poor healthcare services.
Corruption in Healthcare: The World Health Organization estimates that corruption claims nearly $455 billion annually, which could otherwise extend universal health coverage globally.
In India, this corruption manifests in various forms, including bribery and sextortion, further undermining the healthcare system’s integrity.
Ineffective Responses: Traditional responses to healthcare violence, such as enhancing security and legal measures, have proven inadequate. These knee-jerk reactions fail to address the root causes of the violence.
What does the Justice K. Hema Committee reportsay on the Culture of Assault?
On Sexual Assault and Consent: Instances of sexual assault are not isolated events but are rooted in societal practices that undermine women’s autonomy and consent.
The National Crime Records Bureau reported 31,516 cases of rape in India in 2022, indicating a significant prevalence of sexual violence against women.
The Justice Hema Committee report emphasizes that rape is a manifestation of a culture that views women as objects rather than individuals with rights.
On Workplace Harassment: The Vishaka guidelines established in 1997 aimed to protect women from workplace harassment, leading to the Sexual Harassment of Women at Workplace Act, 2013, which mandates the formation of Internal Complaints Committees (ICC).
The report argues that ICCs are inadequate for the film industry due to potential biases and influence from abusers, advocating for an independent government forum to address these issues.
Need to Rethink Violence in Healthcare:
Understanding the Multi-faceted Nature of Violence: Violence in healthcare settings is not limited to patient assaults on healthcare workers, it also includes institutional and managerial violence. This encompasses horizontal violence among healthcare providers and the systemic issues that create a hostile work environment.
Implementing Comprehensive Safety Measures: While immediate responses such as improving security and legal protections are necessary, they must be part of a broader strategy that includes training healthcare workers on conflict resolution, mental health support, and creating a culture of safety within healthcare institutions.
About Justice J.S. Verma Committee Recommendations
Recommendations on
Explanation
Rape
• It recognized rape as a Crime of Power, not just passion.
• Expand definition to include all forms of non-consensual penetration.
• Remove marital rape exception; marriage should not imply automatic consent. (European Commission of Human Rights in C.R. vs U.K)
Sexual Assault
• Broaden definition to include all non-consensual, non-penetrative sexual acts.
• Penalty: Up to 5 years of imprisonment or fines.
Verbal Sexual Assault
• Criminalize unwelcome sexual threats.
• Punishable by up to 1 year in prison or fines.
Sexual Harassment at Workplace
• Include domestic workers under protections.
• Replace internal complaint committees with Employment Tribunals.
• Employers to compensate victims of sexual harassment.
Acid Attacks
• Propose a 10-year minimum punishment, separate from grievous hurt.
• Establish a compensation fund for victims.
Women in Conflict Areas
• Review AFSPA; exclude government sanction for prosecuting sexual offenses by armed forces.
• Appoint special commissioners to monitor offenses.
Trafficking
• Comprehensive anti-trafficking laws beyond prostitution.
• Protective homes for women and juveniles overseen by High Courts.
Child Sexual Abuse
• Define ‘harm’ and ‘health’ in the Juvenile Justice Act to include both physical and mental aspects.
Death Penalty
• Opposed chemical castration and death penalty for rape.
• Recommend life imprisonment.
Medical Examination of Rape Victims
• Ban the two-finger test; victim’s past sexual history should not influence the case.
Reforms in Case Management
• Set up Rape Crisis Cells, increase police accountability, allow online FIR filing.
• Encourage community policing and increase police personnel.
Need for a Comprehensive Approach:
National Task Force: Improving hospital security and infrastructure alone may not be sufficient to address the problem. The national task force constituted by the Supreme Court should devise a comprehensive road map to prevent and arrest medical corruption, particularly in the public sector.
Need Expertise: The task force should include experts from public health, medico-legal, and other allied fields, along with the participation of the larger governing and administrative community.
Note: Recently some states have taken steps to empower women. For example, the Himachal Pradesh Assembly passed a Bill on Tuesday to increase the minimum marriage age for women from 18 to 21 years.
Mains PYQ:
Q Appropriate local community level healthcare intervention is a prerequisite to achieve ‘Health for All’ in India. Explain. (UPSC CSE 2018)
Q We are witnessing increasing instances of sexual violence against women in the country. Despite existing legal provisions against it, the number of such incidences is on the rise. Suggest some innovative measures to tackle this menace. (UPSC CSE 2014)
The Supreme Court of India denied permission to the parents of Harish Rana, a 32-year-old man in a vegetative state for 11 years, to remove his Ryles tube which is a device used for feeding.
A Ryles tube, also known as a nasogastric (NG) tube, is a medical device used for various purposes related to nutrition and gastric management. It is inserted through the nose, passing through the nasal cavity, down the esophagus, and into the stomach.
Recent Supreme Court Judgment:
The Bench headed by CJI D.Y. Chandrachud observed that the Ryles tube is not a life support system and therefore could not be withdrawn.
This decision has stirred legal and ethical debates, as the Supreme Court’s 2018 judgment permits the withdrawal of life support in terminal cases under the concept of “passive euthanasia.”
Passive euthanasia involves the withdrawal of medical treatment with the intention of hastening the death of a terminally ill patient.
The Supreme Court initially legalized this practice in 2018, allowing patients to create a “living will” to refuse life-sustaining treatment when they are unable to communicate their wishes.
Ethical Challenges:
Question of whether the decision benefits the patient: The judgment raises concerns about whether the decision benefits the patient, as prolonging life in such a condition may increase suffering.
Prolonged suffering: The principle of not causing harm is challenged since keeping the patient in a vegetative state with artificial feeding may lead to prolonged suffering for both the patient and their caregivers.
Against Right to Life and Death: The patient’s rights to a dignified life and death may be compromised which is addressed in various judgments like Common Cause v. Union of India (2018). This judgment recognised the right to die with dignity as part of the right to life under Article 21.
Autonomy: The patient’s right to choose, which is central to the concept of dignity, has been overlooked. The judgment did not consider the wishes of the patient or their family in determining the course of action.
Need for Legal Clarity:
Distinguishing Euthanasia from Withdrawal of Life Support: There is a pressing need to legally clarify the difference between euthanasia and the withdrawal of futile life-sustaining interventions.
Involvement of Medical and Ethical Experts: The decision-making process in such sensitive cases should involve palliative care physicians and ethical experts to ensure that medical and ethical considerations are fully addressed.
Advance Care Planning: Promoting Advance Medical Directives and Advance Care Planning is crucial to empower individuals to have control over their end-of-life decisions, ensuring that their rights to a good quality of life and death are respected.
Systemic Reforms: The judgment highlights the need for systemic reforms to avoid forcing families into legal battles and to ensure that patients’ rights are safeguarded with appropriate legal frameworks.
Conclusion: The recent Supreme Court judgment highlights the urgent need for legal clarity, ethical considerations, and systemic reforms to protect patient rights and ensure dignity in end-of-life decisions.
Mains question for practice:
Q Discuss the need for legal clarity and systemic reforms to uphold the dignity and rights of patients in end-of-life decisions. (150 words) 10M
India’s healthcare since globalization has improved greatly, and is globally recognized due to skilled professionals, effective policies, and strong institutions which draw patients from over 147 countries.
Economic implications of being a preferred Medical Destination:
Foreign Exchange Savings: India saves billions in foreign exchange as fewer Indians need to travel abroad for advanced medical treatments.
Revenue Generation: The influx of international patients generates over $9 billion annually, contributing to economic growth.
Job Creation: The medical tourism sector creates employment opportunities in healthcare, hospitality, transportation, and pharmaceuticals.
Cost-Effective Treatments: India’s affordable yet high-quality medical services attract patients globally, further boosting the economy.
What are the challenges?
Shortage of Healthcare Professionals
Current Shortage: India is estimated to be short of around 600,000 doctors, leading to a doctor-patient ratio of approximately 0.7 doctors per 1,000 people, which is significantly lower than the World Health Organization’s recommended ratio of 1 doctor per 1,000 people.
Future Demand: By 2030, the demand for healthcare professionals in India is expected to double, driven by an ageing population and the increasing burden of non-communicable diseases.
Inadequate Public Healthcare Spending
Low Expenditure: As of 2021-22, India’s public healthcare expenditure stood at 2.1% of GDP, which is significantly lower than that of many developed countries, For instance, countries like Japan and France spend about 10% of their GDP on healthcare, while the United States spends 16.9%.
Comparison with Neighbors: Even neighbouring countries like Bangladesh and Pakistan allocate over 3% of their GDP to public healthcare.
Unequal Access to Healthcare
Urban-Rural Disparity: There is a stark disparity in healthcare access between urban and rural areas. Rural regions often lack basic healthcare facilities, leading to limited access to quality services for a significant portion of the population.
Healthcare Infrastructure: India’s healthcare infrastructure is inadequate to meet the growing demands of its population. For instance, India has one of the lowest per capita bed counts in the world, with only about 0.5 hospital beds per 1,000 people, compared to the OECD average of 4.7 beds per 1,000 people.
High Out-of-Pocket Expenditure
Financial Burden: Approximately 75% of healthcare expenditure in India is borne out-of-pocket by individuals and families.
Need for a Strong Vision (Way forward)
“Heal in India” Initiative: The Prime Minister’s vision of “Heal in India” emphasizes positioning India as a global healthcare leader. This initiative is not merely a slogan but a strategic approach to enhance India’s reputation as a preferred medical destination.
Youth Engagement: Inspiring the youth to pursue careers in healthcare is crucial for sustaining growth in this sector. By encouraging innovation and entrepreneurship among young Indians, the country can ensure a robust healthcare system.
Investment in Public Healthcare: Increase public healthcare spending to improve infrastructure, especially in rural areas, and bridge the urban-rural disparity.
Focus on Medical Device Manufacturing: Promote domestic production of medical devices under the “Make in India” initiative to reduce dependency on imports.
Mains PYQ:
Q Appropriate local community-level healthcare intervention is a prerequisite to achieve ‘Health for All’ in India. Explain. (UPSC IAS/2018)
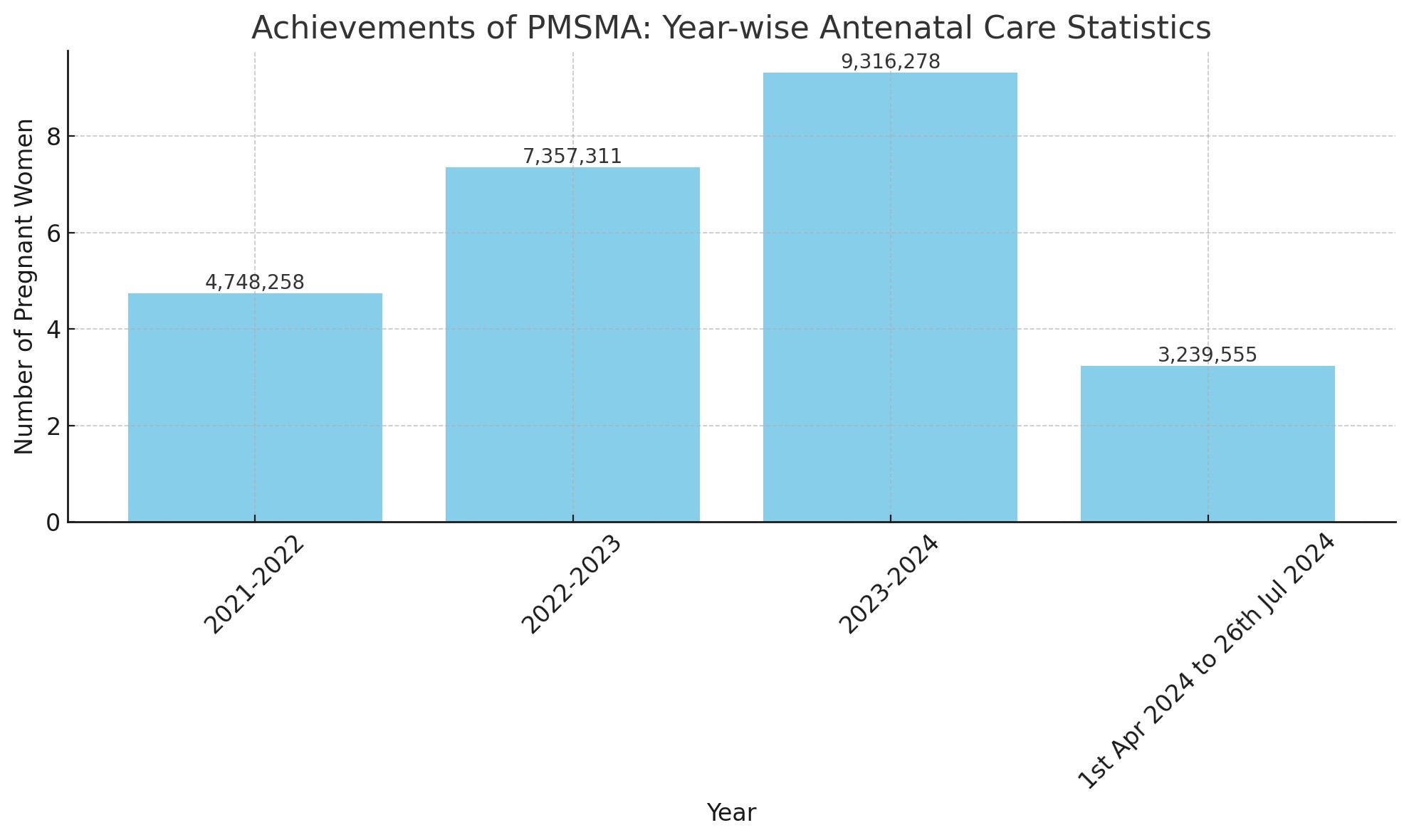
An Extended Pradhan Mantri Surakshit Matritva Abhiyan (E-PMSMA) strategy was launched to ensure quality Antenatal Care (ANC) for pregnant women.
The strategy focuses on individual tracking of high-risk pregnancies (HRP) and provision of additionalPMSMA sessions beyond the 9th of every month.
AboutHigh-Risk Pregnancy:
A high-risk pregnancy involves greater risk of health complications for the mother, the foetus, or both, due to pre-existing medical conditions, conditions that develop during pregnancy, or foetal issues.
Common Factors:
Maternal Health Conditions: Pre-existing diabetes, hypertension, HIV, kidney disease, or conditions arising during pregnancy like gestational diabetes and preeclampsia.
Obstetric Factors: Previous caesarean section, history of preterm labor, multiple pregnancies, and congenital malformations.
About Pradhan Mantri Surakshit Matritva Abhiyan (PMSMA)
Details
About
An initiative to provide quality antenatal care (ANC) to all pregnant women.
Launch
October 2016
Target Group
All pregnant women, especially those in their second and third trimesters.
Frequency
Services provided on the 9th of every month at government health facilities.
Objective
Ensure safe motherhood by providing comprehensive and quality antenatal care universally.
Key Functions
General Check-Up: Physical and clinical examinations by medical professionals.
Laboratory Investigations: Routine blood tests, urine tests, and other necessary laboratory investigations.
Ultrasound: Ultrasound examination to monitor foetal growth and development.
Counseling: Nutritional and lifestyle counseling to ensure a healthy pregnancy.
High-Risk Identification: Screening and identification of high-risk pregnancies and appropriate referrals for specialized care.
Key Features
Free of Cost: All services under PMSMA are provided free of cost.
Fixed Day ANC Services: Antenatal care services are provided on a fixed day every month.
Lab Investigations: Basic investigations like Hb, urine albumin, RBS, malaria test, VDRL test, blood grouping, CBC, ESR, and USG.
Public-Private Partnership: Encourages participation of private sector healthcare providers in providing ANC services.
Incentives: Incentives for healthcare providers who participate in the program.
Categorization of Pregnant Women
Green Sticker – for women with no risk factor detected
Red Sticker – for women with high risk pregnancy
BlueSticker – for women with Pregnancy Induced Hypertension
YellowSticker – pregnancy with co-morbid conditions such as diabetes, hypothyroidism, STIs
Benefits
Improved Maternal Health: Regular and comprehensive ANC helps in early detection and management of complications, improving maternal health outcomes.
Reduced Mortality Rates: Timely and quality care reduces maternal and infant mortality rates.
Health Education: Provides health education and counseling to pregnant women, promoting better health practices.
High-Risk Management: Identifies and manages high-risk pregnancies effectively, ensuring specialized care for those who need it.
PYQ:
[2024] With reference to the ‘Pradhan Mantri Surakshit Matritva Abhiyan’, consider the following statements:
1. This scheme guarantees a minimum package of antenatal care services to women in their second and third trimesters of pregnancy and six months post-delivery health care service in any government health facility.
2. Under this scheme, private sector health care providers of certain specialities can volunteer to provide services at nearby government health facilities.
Which of the statements given above is/are correct?
Q1 COVID-19 pandemic has caused unprecedented devastation worldwide. However, technological advancements are being availed readily to win over the crisis. Give an account of how technology was sought to aid the management of the pandemic. (UPSC IAS/2020)
Q2 Critically examine the role of WHO in providing global health security during the Covid-19 pandemic. (UPSC IAS/2020)
Note4Students:
Mains: Reasons behind the disagreement on the Pandemic Treaty;
Mentor comments: Despite extensive negotiations, 194 WHO member states failed to finalize a historic Pandemic Agreement to bolster global pandemic preparedness and reduce inequities highlighted by COVID-19. At the 77th World Health Assembly (May 27-June 1, 2024), two significant developments occurred. First, amendments to the International Health Regulations (IHR) 2005 were agreed upon, drawn from 300 global reform proposals. These amendments aim to improve response to Public Health Emergencies of International Concern (PHEIC) and introduce a Pandemic Emergency (PE) category, ensuring equitable access to health products and financial support for developing countries, emphasizing solidarity and equity, and mandating a National IHR Authority.
Let’s learn!
__
Why in the News?
The 77th World Health Assembly in May 2024 failed to finalize the treaty due to disagreements on key articles, particularly PABS, technology transfer, and the One Health approach.
Background:
The COVID-19 pandemic exposed severe limitations in the International Health Regulations (IHR) and the WHO’s institutional capacities to effectively prevent, prepare for and respond to global health emergencies.
In light of the pandemic’s devastating global impact, many countries called for a stronger international framework to deal with future pandemics.
Responding to these calls, a special session of the World Health Assembly (WHA) in November 2021 agreed to establish an intergovernmental negotiating body (INB) to draft and negotiate a WHO convention, agreement or other international instrument on pandemic prevention, preparedness and response
What is the Pandemic Treaty?
The Pandemic Treaty, also known as the International Treaty on Pandemic Prevention, Preparedness and Response, is a proposed international agreement currently being negotiated by the 194 member states of the World Health Organization (WHO).
Key Provisions
Pathogen Access and Benefit Sharing (PABS): The treaty aims to establish a PABS system to ensure that genetic resources and pathogen samples shared from developing countries are reciprocated with corresponding benefits, such as vaccines and diagnostics.
Technology Transfer and Intellectual Property: The treaty seeks to address issues related to technology transfer, local production, and intellectual property rights to enhance the manufacturing capacities of low- and middle-income countries.
One Health Approach: The treaty emphasizes a holistic approach that recognizes the interconnections between human, animal, and environmental health, promoting coordinated public health measures across these domains.
Reasons behind the disagreement
Pathogen Access and Benefit Sharing (PABS): The PABS mechanism under Article 12 is a central point of contention, with low- and middle-income countries (LMICs) advocating for guaranteed access to at least 20% of shared pandemic products.
In contrast, many high-income countries argue that this percentage should be the maximum limit, with some refusing to agree to any fixed percentage.
Technology Transfer and Intellectual Property: Disagreements over technology transfer provisions are significant, with LMICs pushing for mandatory technology transfer and intellectual property waivers to enable local production of vaccines and treatments.
High-income countries prefer voluntary agreements, fearing that mandatory requirements could undermine their intellectual property rights.
One Health Approach: The One Health approach, which emphasizes the interconnectedness of human, animal, and environmental health, has faced resistance from LMICs. They view it as an additional burden without adequate funding, while high-income countries strongly support it.
Geopolitical Discord: Geopolitical tensions and competing interests between higher- and lower-income countries have hindered progress in negotiations.
Misinformation and Distrust: The negotiations have been affected by misinformation, skepticism, and distrust among member states. Some countries are concerned about the implications of the agreement on their national sovereignty and public health policies.
Urgency vs. Comprehensive Solutions: There is a tension between the urgency to finalize an agreement and the desire to address complex issues comprehensively. Some countries are pushing for quick resolutions, while others emphasize the need for thorough discussions to ensure long-term effectiveness.
Way forward:
Promote Inclusive Dialogue and Mutual Compromise: Need to facilitate continuous, transparent dialogue among all member states to address concerns and build trust. Encourage mutual compromise by balancing the interests of both high- and low-income countries, ensuring that all parties feel their needs and perspectives are being considered.
Strengthen Financial and Technical Support for LMICs: Need to enhance financial and technical assistance for low- and middle-income countries to implement the proposed treaty provisions effectively.
PYQ Relevance: Mains: Q1 Public health system has limitation in providing universal health coverage. Do you think that private sector can help in bridging the gap? What other viable alternatives do you suggest?(UPSC IAS/2015) Q2 What do you understand by nanotechnology and how is it helping in health sector? (UPSC IAS/2020)
Prelims: Q Doctors Without Borders (Medecins Sans Frontieres)’, often in the news, is: (a) a division of World Health Organization (b) a non-governmental international organization (c) an inter-governmental agency sponsored by European Union (d) a specialized agency of the United Nations
Note4Students:
Mains:Challenges related to Homeless individuals;
Mentor comments: Socio-normative representations of homeless persons living with mental illness (HPMI) often depict them as refuge seekers, leading to interventions focused on transferring them to mental hospitals or shelters. This perspective assumes that displacement from the streets is necessary due to associated risks, which, while valid, oversimplifies their complex realities. Such representations result in coercive measures that fail to recognise the agency of HPMI, perpetuating a cycle of institutionalization rather than fostering genuine community reintegration and support. Addressing these representations is crucial for developing more effective and respectful care strategies.
Let’s learn!
__
Why in the News?
Homeless individuals with mental illness are often viewed as needing rescue, leading to their forced relocation to hospitals or shelters, despite the debatable risks of street living.
Efforts at Integration
Collaborative Initiatives in India: The collaboration among various organizations, including the National Health Mission and local civil society groups, has facilitated access to emergency care and recovery centers (ECRCs) in district hospitals, improving support for homeless persons with mental illness (HPMI).
Breaking Down Asylum Models: The integration of services aims to dismantle the traditional asylum model, which often perpetuates negative stereotypes about mental illness, by providing more immediate and localized care.
Last-Mile Proximal Care: The establishment of ECRCs ensures that care reaches individuals in scattered geographies, addressing the immediate needs of those experiencing crises.
Transformative Care Models: Thefocus on smaller care units that are adequately staffed emphasizes personal attention and the management of comorbidities, which is essential for those facing prolonged adversities.
Problems with institutional spaces:
Long-Term Custodial Care: Approximately 37% of individuals in state psychiatric facilities have long-term needs, with many having histories of homelessness. The median duration of stay is six years, indicating a reliance on institutional care rather than effective community reintegration.
According to the World Health Organization, mental disorders account for 10.6% of total disability among older adults.
Rigid Discharge Criteria: Discharge criteria for individuals in psychiatric facilities are often overly simplistic, leading to inadequate support for those transitioning back to community life.
Isolation from Social Resources: Institutional settings create barriers to accessing social resources and community participation, leading to social isolation and a lower quality of life.
Mental Health America reports that over half (54.7%) of adults with mental illness do not receive treatment, often due to such barriers.
Ineffective Rehabilitation Models: Current rehabilitation models often default to custodial care, failing to promote innovative, community-based solutions.
Initiatives like Housing First and the ‘Home Again’ collaborative in India demonstrate the feasibility of comprehensive social and clinical care, yet traditional models continue to limit the potential for improved outcomes for individuals with mental health challenges.
Way forward:
Shift from Paternalistic to Liberatory Strategies: The need to take social protection measures for homeless people with mental illness (HPMI) must transition from paternalistic interventions to liberatory-focused strategies that honour individual agency.
This includes implementing a modest monthly disability allowance of ₹1,500 to provide financial support while addressing bureaucratic barriers to accessing essential documentation like Aadhar and banking services.
Holistic and Imaginative Approaches: Supportive measures must be complemented by imaginative and holistic strategies that address structural issues such as discrimination, violence, and social segregation.
![[29th July 2024] The Hindu Op-ed: Recasting care models for mental illness, homelessness](https://www.civilsdaily.com/wp-content/uploads/2024/07/29-july-1568x882.jpg)