As Dr. B.R. Ambedkar said, “Political democracy cannot last unless there lies at the base of it social democracy.” Development and welfare schemes are pivotal for uplifting vulnerable sections of society.
Welfare Schemes – “Discriminatory”
Targeted Beneficiaries – Eg- Stand-Up India provides loans only to SC/ST and women entrepreneurs.
Resource Allocation Bias – Eg- Special Component Plan (SCP) and Tribal Sub-Plan (TSP) earmark fixed budgetary percentages.
Political and Regional Disparities – Eg- 90% central funding to North East and Special Category states under CSS
Dependency and Moral Hazard – Overemphasis on welfare transfers can foster dependency rather than empowerment.
Bias and Perceived Discrimination – Non-reserved categories view these schemes as diluting meritocracy and unfair. Eg- Reservation Policies
Welfare Schemes – Corrective, Not Discriminatory
Constitutional Mandate for Positive Discrimination – Articles 15(4) and 46 empower the state to make special provisions for the advancement of socially and educationally backward classes.
Bridge Structural Inequalities and corrects historical injustices. Eg- 106th Amendment Act
Inclusive Human Development – Programs like Ayushman Bharat, PM Poshan, and PM Matru Vandana Yojana address basic capabilities of health, nutrition, and education.
Aligns with the UN SDGs (Goal 1: No Poverty, Goal 10: Reduced Inequality) which encourage special focus on vulnerable populations.
Resource Optimization- Limited resources necessitate prioritizing those most in need, ensuring efficient use of funds.
Impact Maximization- Eg- Pradhan Mantri Awas Yojana (PMAY) for affordable housing.
Social Cohesion- Inclusive growth fosters social stability and reduces tensions arising from socio-economic disparities.
Impact
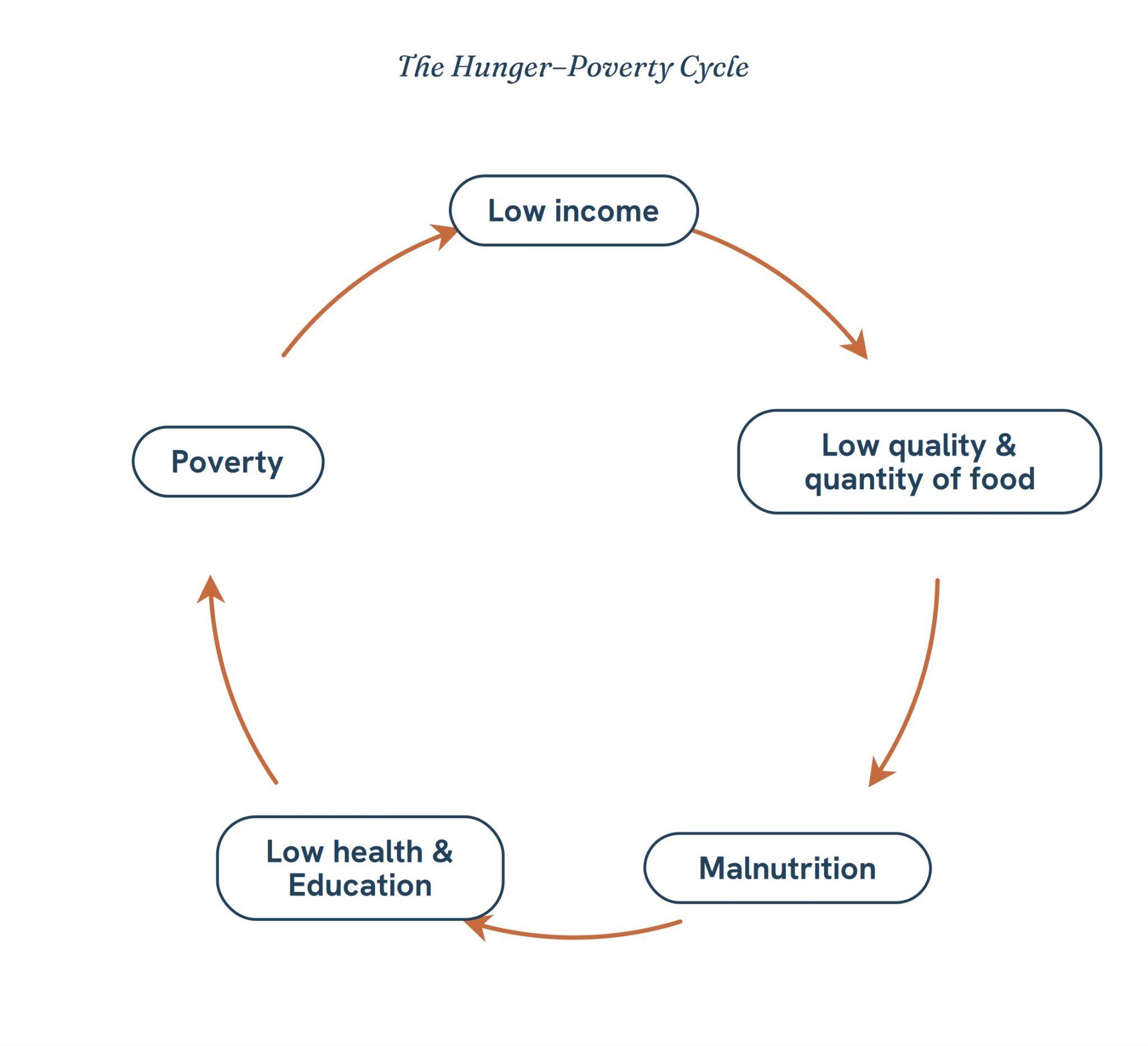
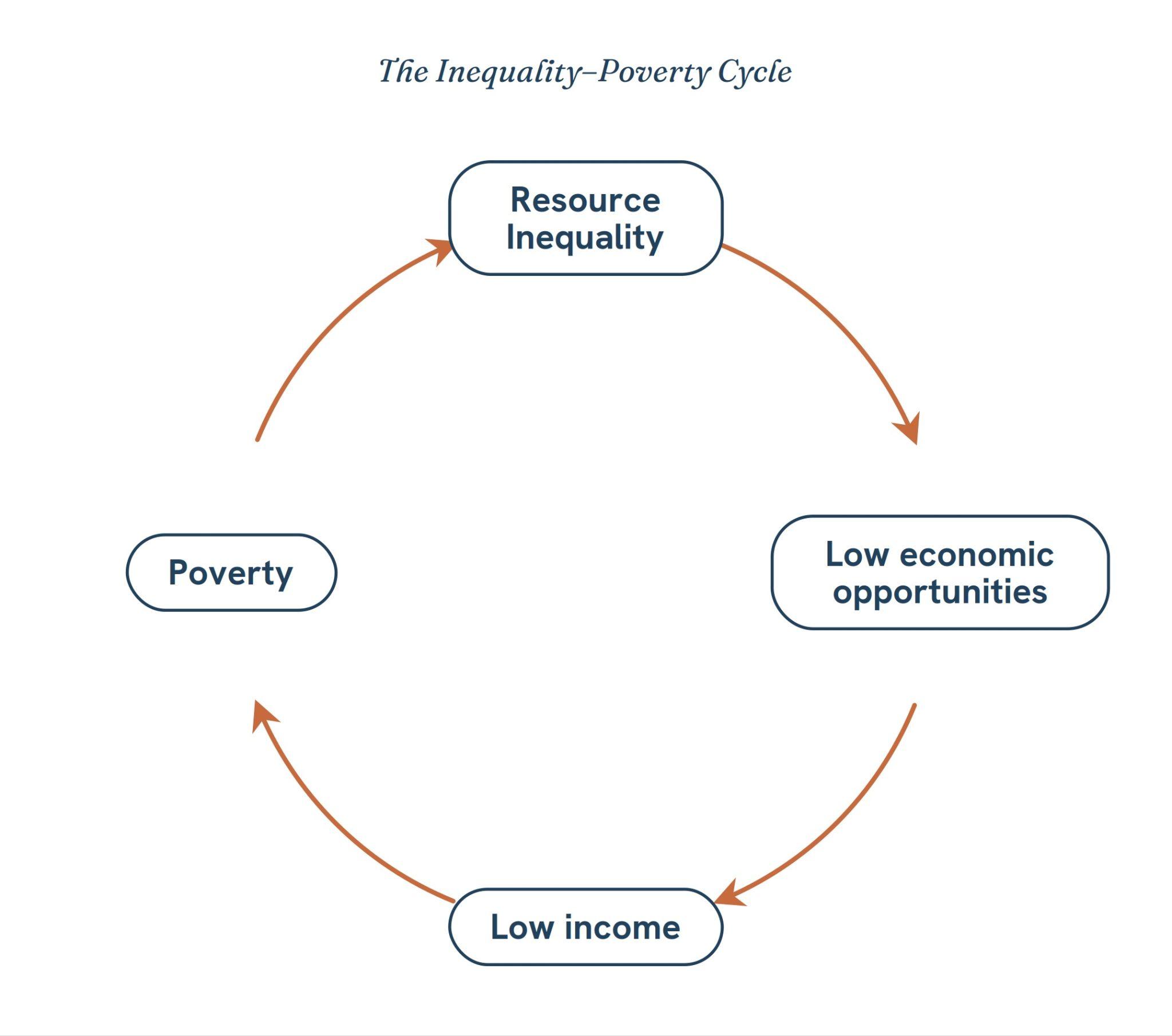
India lifted 248 million people out of multidimensional poverty between 2013-14 and 2022-23 (NITI Aayog, MPI Report 2024).
MGNREGA: Women’s participation stands at over 57%, reflecting strong gender inclusion.
PM Ujjwala Yojana – Over 10.5 crore LPG connections provided since 2016
PM Jan Dhan Yojana: 55 crore accounts opened, with 56% held by women
Way Forward
Capability Approach: increase expenditure on Health (2.5% of GDP) and Education (6% of GDP)
Bottom-up Planning – Porto Alegre Brazil Model
Welfare schemes for the vulnerable may appear discriminatory in form, but they are affirmative in purpose to realise the vision of “Sabka Saath, Sabka Vikas, Sabka Vishwas”