Why in the news?
This year’s theme for International Fatty Liver Day, an awareness initiative observed annually in June, is ‘Act Now, Screen Today’. This theme holds more urgency now than ever before.
Liver Diseases in recent times
|
India’s Growing Burden of Fatty Liver Disease
Note: MASLD, or Metabolic dysfunction-associated steatotic liver disease, is a reclassification of what was previously known as non-alcoholic fatty liver disease (NAFLD).
- High Prevalence Rates: The global prevalence of Metabolic dysfunction-associated steatotic liver disease (MASLD) is estimated at 25-30%. In India, a 2022 meta-analysis revealed that the pooled prevalence of fatty liver among adults was 38.6%. Among obese children in India, the prevalence was around 36%.
- Progression of Disease: The continuous damage caused by fatty liver leads to more severe conditions such as steatohepatitis and cirrhosis, often requiring liver transplants.
Causes of Growing Burden of Fatty Liver Disease
- Lack of Early Detection: Fatty liver disease often goes undetected in early stages due to lack of symptoms. Diagnosis usually occurs at an advanced stage, when significant liver damage has already taken place.
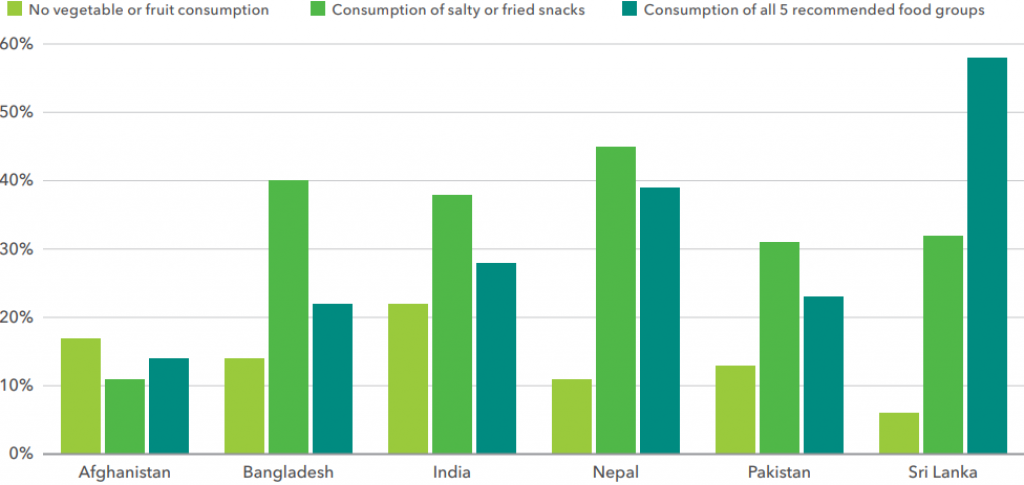
- Diet and Insulin Resistance: Excessive consumption of carbohydrates, especially refined carbs and sugars, leads to metabolic problems. High carbohydrate intake results in persistently high insulin levels and insulin resistance, promoting the conversion of excess glucose into fatty acids, which are then stored in the liver.
Initiatives Taken by the Government
- Integration with NPCDCS: The Ministry of Health & Family Welfare launched operational guidelines for integrating NAFLD with the National Programme for Prevention & Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) in February 2021.
- Health Promotion and Prevention: The Ayushman Bharat- Health and Wellness Centres (AB-HWCs) are being used to promote healthy living and screen for hypertension, diabetes, and other common NCDs.
Personalization is the Key
- Tailored Screening Tests: The selection of screening tests and their frequency should be based on individual risk factors, including family history, lifestyle, and pre-existing health conditions.
- Avoiding Generic Assumptions: Clinicians should not rely solely on age or physical markers; instead, they should consider a comprehensive risk profile. Non-communicable diseases are increasingly affecting diverse populations, including children.
- Integrated Health Strategies: Combining dietary modifications, regular physical activity, and effective weight management to mitigate liver disease risks.
- Frequent Screenings: Regular monitoring of liver health through non-invasive tools like vibration-controlled transient elastography. Continuous assessment of liver stiffness to detect early stages of liver fibrosis and monitor treatment responses.
- Active Health Management: Emphasis on the importance of individuals taking control of their health by being aware of their diet and lifestyle choices.Encouragement of frequent health screenings to detect and manage liver disease early.
Way Forward:
- Awareness Campaigns: Government initiatives focus on raising awareness about the importance of liver health and the risks associated with MASLD.
- Health Screenings: Programs promoting comprehensive health screenings that include physical examinations, blood tests, and abdomen ultrasounds to detect liver diseases early.
Mains PYQ
Q The public health system has limitations in providing universal health coverage. Do you think that the private sector can help in bridging the gap? What other viable alternatives do you suggest? (UPSC IAS/2015)
![[7th June 2024] The Hindu Op-ed: Health regulations need a base-to-top approach](https://www.civilsdaily.com/wp-content/uploads/2024/06/7-June-2nd-1568x882.jpg)