The draft NEP (National Education Policy) document points out that close to five crore children currently in elementary school do not have foundational literacy and numeracy skills.
Severe learning crisis: The document cites several possible reasons for this crisis.
First reason: Many children enter school before age six.
Lack of options: This is partly due to the lack of affordable and accessible options for pre-schooling.
Therefore, too many children go to Std. I with limited exposure to early childhood education.
Consequences for the poor: Children from poor families have a double disadvantage -lack of healthcare and nutrition and the absence of a supportive learning environment on the other.
Second reason: Lack of developmentally appropriate activities by age and phase.
The misplaced focus of ICDS: School readiness or early childhood development and education activities have not had a high priority in the ICDS system.
Acting as an extension of pre-school education: Private preschools that have increased access to preschool but are often designed to be a downward extension of schooling.
Thus, they bring in school-like features into the pre-school classroom, rather than developmentally appropriate activities by age and phase.
Three clear trends in ASER-2019 data
First trend: Scope for expansion of Anganwadi network.
Expansion network: There is considerable scope for expanding Anganwadi outreach for three and four-year-old children.
All-India data from 2018 shows that slightly less than 30 per cent children at age three and 15.6 per cent of children at age four are not enrolled anywhere.
Second trend: Under 6 students in class I.
ASER 2018 data show that 27.6 per cent of all children in Std I are under six.
It is commonly assumed that children enter Standard I at age six and that they proceed year by year from Std I to Std VIII.
The Right to Education Act also refers to free and compulsory education for the age group six to 14.
However, the practice on the ground is quite different.
Third trend: There are important age implications for children’s learning.
Association with learning output: ASER-2019 indicate the higher learning output associated with age in the same class.
In Std. I, the ability to do cognitive activities among seven-eight-year olds can be 20 percentage points higher than their friends who are five years old but in the same class.
In terms of reading levels in Std. I, 37.1 per cent children who are under six can recognise letters whereas 76 per cent of those who are seven or eight can do the same.
Age distribution in Std. I vary considerably between government and private schools.
Private schools in many states have a relatively older age distribution.
Way forward
Understanding the children: Understanding the challenges that children face when they are young is critical if we want to solve these problems early in children’s life.
Providing for developmentally appropriate skill: Instead of focusing on the pre-school years as the downward extension of school years there is a need for providing developmentally appropriate skill in these years.
Pedagogy: On the pedagogy side reworking of curriculum and activity is urgently needed for entire age band of four to eight.
The Union Ministry of Health and Family Welfare has published a national policy for the treatment of 450 ‘rare diseases’.
About the Policy
The Centre first prepared such a policy in 2017 and appointed a committee in 2018 to review it.
It was created on the direction of the Delhi High Court to the Ministry of Health and Family Welfare.
This was in response to writ petitions for free treatment of such diseases, due to their “prohibitively” high cost of treatment.
Hence, a policy was deemed necessary to devise a “multipronged” and “multisectoral” approach to build India’s capacity for tackling such ailments.
Why need such a policy?
As per the policy, out of all rare diseases in the world, less than five per cent have therapies available to treat them.
In India, roughly 450 rare diseases have been recorded from tertiary hospitals, of which the most common are Haemophilia, Thalassemia, Sickle-cell anemia, auto-immune diseases, Gaucher’s disease, and cystic fibrosis.
Features of the policy
While the policy has not yet put down a detailed roadmap of how rare diseases will be treated.
It has mentioned some measures, which include creating a patient registry for rare diseases, arriving at a definition for rare diseases that is suited to India, taking legal and other measures to control the prices of their drugs etc.
It intends to kickstart a registry of rare diseases, which will be maintained by the Indian Council of Medical Research (ICMR).
Under the policy, there are three categories of rare diseases — requiring one-time curative treatment, diseases that require long-term treatment but where the cost is low, and those needing long-term treatments with high cost.
Some of the diseases in the first category include osteopetrosis and immune deficiency disorders, among others.
As per the policy, the assistance of Rs 15 lakh will be provided to patients suffering from rare diseases that require a one-time curative treatment under the Rashtriya Arogya Nidhi scheme.
The treatment will be limited to the beneficiaries of Pradhan Mantri Jan Arogya Yojana.
What are rare diseases?
Broadly, a ‘rare disease’ is defined as a health condition of low prevalence that affects a small number of people when compared with other prevalent diseases in the general population. Many cases of rare diseases may be serious, chronic and life-threatening.
While a majority of rare diseases are believed to be genetic, many — such as some rare cancers and some autoimmune diseases — are not inherited, as per the NIH.
According to the policy, rare diseases include genetic diseases, rare cancers, infectious tropical diseases, and degenerative diseases.
Definition
India does not have a definition of rare diseases because there is a lack of epidemiological data on its incidence and prevalence.
While there is no universally accepted definition of rare diseases, countries typically arrive at their own descriptions, taking into consideration disease prevalence, its severity and the existence of alternative therapeutic options.
In the US, for instance, a rare disease is defined as a condition that affects fewer than 200,000 people.
The same definition is used by the National Organisation for Rare Disorders (NORD) in India.
The Annual Status of Education Report (ASER) 2019 (rural) was recently released by NGO Pratham.
Highlights of the report
Only 16% of children in Class 1 in 26 surveyed rural districts can read text at the prescribed level, while almost 40% cannot even recognise letters.
Only 41% of these children could recognise two digit numbers.
Private schools ahead
Of six-year olds in Class 1, 41.5% of those in private schools could read words in comparison to only 19% from government schools.
Similarly, 28% of those in government schools could do simple addition as against 47% in private schools.
This gap is further exacerbated by a gender divide: only 39% of girls aged 6-8 are enrolled in private schools in comparison to almost 48% of boys.
The report also found that a classroom could include students from a range of age-groups, skewing towards younger children in government schools.
Determinants of learning outcomes
The ASER report shows that a large number of factors determine the quality of education received at this stage, including the child’s home background, especially the mother’s education level; the type of school, whether anganwadis, government schools or private pre-schools; and the child’s age in Class 1.
More than a quarter of Class 1 students in government schools are only 4 or 5 years old, younger than the recommended age.
The ASER data shows that these younger children struggle more than others in all skills.
Permitting underage children into primary grades puts them at a learning disadvantage which is difficult to overcome,” said the report.
Role of Mothers
Among the key findings of ASER 2019 is that the mother’s education often determines the kind of pre-schooling or schooling that the child gets.
The report says that among children in the early years (ages 0-8), those with mothers who had completed eight or fewer years of schooling are more likely to be attending anganwadis or government pre-primary classes.
With 75% women in the productive age group not in the workforce, they can be better engaged in their children’s development, learning and school readiness.
Key suggestions made by the report
ASER found that the solution is not to spend longer hours teaching children the 3Rs.
Counter-intuitively, the report argues that a focus on cognitive skills rather than subject learning in the early years can make a big difference to basic literacy and numeracy abilities.
The survey shows that among Class 1 children who could correctly do none or only one of the tasks requiring cognitive skills, about 14% could read words, while 19% could do single digit addition.
However, of those children who could correctly do all three cognitive tasks, 52% could read words, and 63% could solve the addition problem.
Focus on productive learning
ASER data shows that children’s performance on tasks requiring cognitive skills is strongly related to their ability to do early language and numeracy tasks,” says the report.
This suggests that focussing on play-based activities that build memory; reasoning and problem-solving abilities are more productive than an early focus on content knowledge.
Global research shows that 90% of brain growth occurs by age 5, meaning that the quality of early childhood education has a crucial impact on the development and long-term schooling of a child.
The advent of a new tetravalent vaccine against the dengue virus has thrown new light into the evidence-based management of dengue.
Why the holistic approach is needed
Apart from promoting the use of the vaccine, gaining control over dengue will also require a holistic approach that has to include within its ambit vector control and proper case management.
Tetravalent vaccine: The vaccine is tetravalent i.e. it provides protection against all the four types of dengue viruses.
The vaccine confers about 80% protection to children vaccinated between 4 and 16 years of age without any major side effects.
Climatic factors: It is essentially a tropical disease that occurs in the countries around the Equator; hot weather and intermittent rainfall favour the sustenance of Aedes aegypti.
Aedes eggs can remain dormant for more than a year and will hatch once they come in contact with water.
Risk factors: Urbanisation, poor town planning, and improper sanitation are the major risk factors for the multiplication of such mosquitoes.
Aedes eggs can remain dormant for more than a year and will hatch once they come in contact with water.
Aedes mosquitoes cannot fly beyond a hundred meters. Hence, keeping the ambiance clean can help prevent their breeding.
Further, these mosquitoes bite during the daytime, so keeping the windows shut in the day hours is also useful.
What needs to be done?
Source reduction activities: Activities like preventing water stagnation and using chemical larvicides and adulticides.
These chemicals need to be applied in periodic cycles to kill the larvae that remain even after the first spray.
Dealing with the manpower shortage: The number of skilled workers available for such measures is low; many posts in government departments remain vacant despite there being a dire public health need.
Due to this deficiency of manpower, active surveillance is not being done in India, says the National Vector Borne Disease Control Program.
Ending the Under-reporting: Dengue cases are often under-reported due to political reasons and also to avoid spreading panic among the common people. Under-reporting needs to be dealt with.
Increasing coordination: There is a lack of coordination between the local bodies and health departments in the delivery of public health measures.
A comprehensive mechanism is required to address these issues.
Need for epidemiological measures: Any communicable disease needs the epidemiological approach. Singapore uses one successful model of mapping and analysing data on dengue, using Geographical Information System (GIS).
The use of GIS involves mapping the streets with dengue cases for vector densities.
Emphasis on the WHO guidelines: Fluid management in the body is the cornerstone in the management of severe diseases like dengue hemorrhagic fever and dengue shock syndrome.
According to the guidelines, coagulation abnormalities are not due to a reduction in the number of platelets alone.
This is why the WHO recommends fresh whole blood or packed cell transfusion in the event of bleeding.
Caution in using alternative medicine drugs: Modern medicine is not against any complementary medicine; when such a medicine is approved after rigorous testing.
However, in the absence of evidence, the efficacy of such medicines remains in the realm of belief instead of science.
So, medicines like Nilavembu kudineer and papaya leaf extract are only belief based.
Conclusion
The communicable nature of Dengue and its asymptomatic nature requires the holistic approach to successfully tackle the disease.
The deaths of nearly 200 children in Kota, from largely preventable diseases, lays bare the condition of the healthcare system in India.
Where does India stand?
According to UNICEF’s ‘State of World’s Children 2019’ report, India reported the maximum number of deaths of children under five in the world in 2018.
8,82,000 children under five died that year.
That means around 2,416 deaths per day.
The death of children due to largely-preventable illnesses is a matter of serious concern and calls for urgent introspection.
Factors that govern child health
Most of the children who died in Gorakhpur, Muzaffarpur and Kota belong to the lowest strata of the society.
It won’t be wrong to conclude that they were victims of structural violence.
This structural violence is unleashed through a multitude of social, political and economic factors apathy of healthcare professionals, poor health services/infrastructure
And low rates of female literacy, economic inequality, the rigid caste system, social apartheid, lack of political will and patriarchy play role.
As a society, we have stopped looking at the deaths of our citizens through the prism of compassion and concern.
Structural violence influences the nature and distribution of extreme suffering.
What is being done in the wrong way?
The government is considering the takeover of 750 district hospitals by private medical colleges through a public-private partnership (PPP) model.
This, despite ample evidence about the failure of the model in the country’s healthcare system.
Nobel laureate Kenneth Arrow demonstrated that profit and private involvement in healthcare lead to an erosion of trust.
An Individual’s demand for medical services is irregular and unpredictable, the involvement of a private market model for such services can be disastrous.
The U.S.’s experiences in the PPP model in healthcare have shone a light on the deficits in transparency and highlighted the lack of care of vulnerable groups.
Conclusion
What urgently a sincere engagement by the state in matters concerning peoples’ health.
We need to question the government’s priorities in a country where nearly a million children die every year
Death of 100 children in the month of December at a Government Hospital in Kota highlights the state of the public health system in India.
Public health as a political agenda
After the incident of a large number of children in such a short span, Rajasthan CM appealed not to politicise the issue.
But it is high time the issue is in fact politicised.
The issue of public health needs to be pushed at the top of the political agenda.
Citizens must hold political parties accountable for the state of healthcare in the country.
Poor infrastructure
Until the number of deaths crosses a certain threshold the poor state of infrastructure fails to attract the attention of the authorities.
This hospital came to light like Gorakhpur Medical college where scores of children had died only after media reports of 963 child deaths.
Conclusion
Every single death in a hospital ought to be seen as a failure that needs to be addressed urgently. For that, the government needs to make public health a priority.
At the End TB summit, 2018 the prime minister of India made a bold commitment to end tuberculosis by 2025-five years ahead of the global target. Which is possible to achieve if the efforts are put at the level it was done in case of polio.
The toll taken by TB
Despite the disease being fully curable, people still die from it.
TB usually affects people in their most productive years and drives families into debt.
It has a direct link to human suffering, discrimination and also poverty.
Due to its infectious spread, it directly affects our economic growth as well.
With resilience, sufficient investment, innovative approaches and strategies and the participation of all stakeholders, TB can be defeated.
First Step- Awareness
The first step is the creation of awareness and empowering of communities.
TB affects millions, yet very few know enough about it.
Multilingual, multi-stakeholder awareness effort to ensure that all Indians knows about the challenges of TB and where to seek treatment is required.
With the expansion of the media and evolving technology, it is possible to reach everyone with the right information.
Second Step- Access to diagnosis and treatment
Ensuring that every Indian get access to correct diagnosis and treatment for TB, regardless of their ability to pay for it is the second step.
To do so, working with the private sector is necessary as was done in the case of polio.
There are numerous innovative private-sector programmes and partnership schemes for TB.
Role of Private sector
Recently launched programmes for doctors and labs offer the private sector various incentives.
Even today, about half a million TB cases go unnotified, especially those seeking care in the private sector.
Those cases need to be tracked and ensured that everyone in the need of treatment and care gets it.
Organisations like Indian Medical Association and Indian Academy of Paediatrics are working with the private sector to ensure patient-centric care as per “Standards of TB Care in India” (STCI).
Drug-resistant TB
A key challenge is building a forward-looking plan to address and control drug resistance.
Drug-resistant TB is a man-made menace that is a major roadblock in a fight against TB.
Every TB patient must be tested for drug resistance at the first point of care, whether in the public or private sector, to rule out any drug resistance.
Efforts by the government
Nikshay Poshan Yojana -in which TB patients receive Rs 500 every month while on treatment was launched.
Nikshay Poshan Yojana ensure that the patients have economic support and nutrition during the required period.
‘TB Harega Desh Jeetega Campaign’ was launched to accelerate the efforts to end TB by 2025.
The campaign aims to initiate preventive and promotive health approaches.
By applying “multi-sectoral and community-led” approach, the government is building a national movement to end TB by 2025.
Resource allocation towards the TB Elimination Programme has been increased by four-fold.
Sincere efforts need to be made to make our health systems more accessible and reliable.
It also required to ensure that those seeking care trust the healthcare system and get the appropriate care for completing treatment.
There is a need to create more labs, point of care tests, an assured drug pipeline, access to new drugs.
The government should also ensure counselling and support for those affected.
Every patient who is diagnosed late and does not receive timely treatment continues to infect others.
To break this cycle, government machinery at the field level should work with communities and provide free diagnosis and treatment to every affected individual.
Conclusion
With all the efforts, planning and resource put in place to eradicate the menace of TB from India, it is possible to achieve the goal by 2025.
The Rajasthan government has started using satellite communication technology in a big way to enhance the learning outcome in educational institutions and generate awareness about social welfare schemes while giving priority to the five aspirational districts selected by NITI Aayog in the State.
SATCOM
Rajasthan has taken an initiative to provide the facility of receive only terminals (ROT) and satellite interactive terminals (SIT) for getting the services of subject experts in the government schools and colleges and propagate various schemes in the remote areas with no Internet connectivity.
What are ROT and SIT?
Satellite Interactive Terminal (SIT) is one of the six selected user networks used by CEC-UGC.
It is operating independently with their user terminals anywhere in the main land of India.
It has one main teaching end along with remote SITs and ROTs.
At present, there are over hundred SITs and ROTs under CEC EDUSAT network, installed at various colleges, and Universities across the country.
Back2Basics
EDUSAT
EDUSAT is the first Indian Satellite built exclusively for serving the educational sector. It was launched in September 2004 by the ISRO.
The satellite based distance education system enables virtual classrooms at rural and remote locations across the country.
Consortium for Educational Communication (CEC) has started two-way audio-video communication through EDUSAT network from 5th September 2005.
ISRO set up a nationwide multi-user educational network in its EDUSAT national Ku – band.
The World Health Organisation (WHO) has selected the year 2020 as the international “Year of the Nurse and Midwife”.
Year of the Nurse and Midwife
It was decided in the honour of 200th birthday of Florence Nightingale.
WHO said that nurses and midwives are the people who devote their lives to caring for children and mothers, looking after senior citizens and giving lifesaving immunizations.
The declaration will help to strengthen nursing and midwifery for Universal Health Coverage.
The declaration will also help to endorse “The NursingNow!” a three-year campaign (2018-2020) to improve health globally by raising the status of nursing.
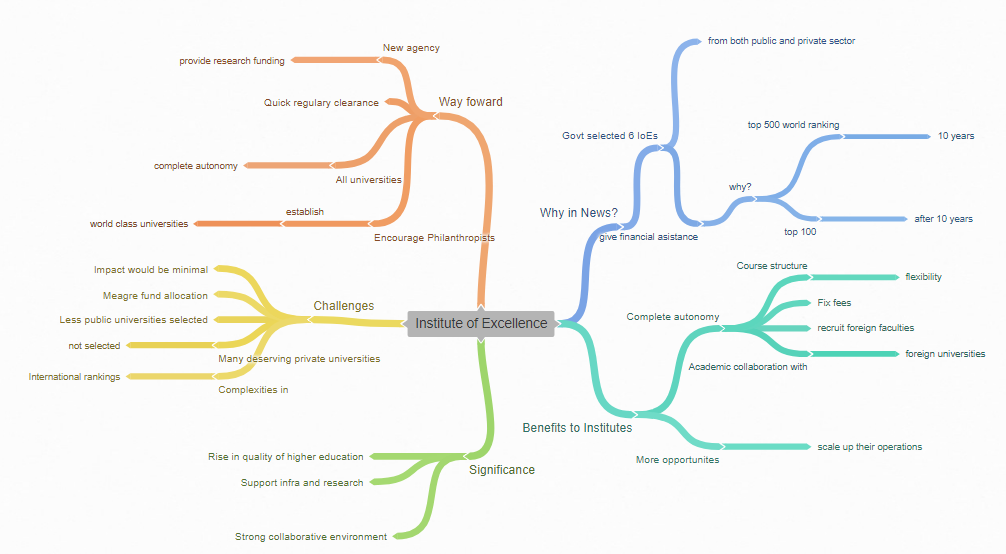
The Government has shortlisted Six Institutions of Eminence (IoEs) including 3 from Public Sector and 3 from Private Sector
It is expected that the above-selected Institutions will come up in the top 500 of the world ranking in 10 years and in top 100 of the world ranking eventually overtime
Each public Institution selected as ‘Institution of Eminence’ will get financial assistance up to Rs. 1000 Crore over the period of five years under this scheme
What will be the benefit of this decision to institutes?
It will ensure complete autonomy to the selected institutions and facilitate them to grow more rapidly
They will get more opportunity to scale up their operations with more skills and quality improvement so that they become World Class Institutions in the field of education
To achieve the top world ranking, these Institutions shall be provided with:
Greater autonomy to admit foreign students up to 30% of admitted students
To recruit foreign faculty up to 25% of faculty strength; to offer online courses up to 20% of its programmes
To enter into academic collaboration with top 500 in the world ranking Institutions without permission of UGC
Free to fix and charge fees from foreign students without restriction
The flexibility of course structure in terms of number of credit hours and years to take a degree
Complete flexibility in fixing of curriculum and syllabus
The significance of this step
IoEs will have unprecedented freedom to fund activities and customise courses, bringing creativity to higher education
It will support infrastructure and research in leading institutions to help them achieve international rankings
Under this initiative, there is recognition that education and research require strong collaborative environments with other institutions and people of diverse nationalities, cultures and ideas.
Criticism/Challenges
1. Less public universities selected:
The committee tasked with recommending Institutes of Eminence (IoE) wanted eight public universities and three private ones to get the tag.
This was from a total of 114 universities that applied for the IoE status and scrutinised by a four-member committee.
These universities included 74 public, 29 private (brownfield) and 11 private (green field) universities. However, the government mysteriously sanctioned only three public universities.
The deserving public ones that missed out are IIT Madras, IIT Kharagpur, Delhi University, Jadavpur University and Anna University
2. Many deserving Private universities not selected:
The deserving private greenfield university applicants that did not make the cut include ISB (Hyderabad), KREA (Raghuram Rajan) and Vedanta. The deserving private universities that did not make the cut include Ashoka University and Amrita University.
3. Very meagre allocation of funds:
The government will give Rs 1,000 crore over five years to each of the three selected public universities.
That is a budgetary outlay of Rs 600 crores per year for all the pomp and show. The top 10 universities in the world spend annually an average of Rs 5,800 crore each on research alone.
The total endowment funds of top 10 universities on an average should be Rs 1,24,000 crore each
4. The impact on the majority of Universities would be minimal:
India currently has approximately 800 universities, 39,000 colleges and 12,000 standalone institutions and over 34 million young Indians join higher education annually. Given the sheer size and scale of the Indian higher education system, the direct benefits that may accrue from implementing this proposal are likely to be minimal.
5. Complexities of International rankings:
The idea of using global rankings for assessing universities has drawn some well-justified criticism before. What does a focus on rankings mean for education? Such rankings tend to prioritise impact of publications over the quality of research programs, the latter being equally, if not more, important for advancing knowledge.
Further, these metrics only speak to individual publications and not the evaluation of research programs or their impact on the communities that they seek to serve.
In nations such as India, where there is a need for research that addresses society, the usability and impact of applied research becomes important, which is one of the goals of creating IoE. This calls for newer, more holistic approaches to assessment of research quality
Way Forward
With the focus trained just on 6 institutes in this particular proposal, several hundreds of government universities where tens of millions of India’s youth study are being laid to waste by excessive regulation, lack of leadership, shortage of teaching staff, inadequate funding, lack of infrastructure and maladministration, especially in smaller cities and towns. This ‘bullet-train’ type solution applied to the education field isn’t necessarily bad, but the lack of transparency seems to only benefit a minuscule proportion of the population in more than one way.
In light of the importance and urgency of transforming India’s higher education system, lessons from around the world, it is clear that there is a better way forward for the nation.
Following steps are required
To unshackle the higher education system quickly and at scale: integrate the regulatory agencies to create a single-window for establishing new universities, eliminate unnecessary functions of these agencies, and realign their responsibilities.
To spur hundreds of universities and thousands of colleges to improve their level of excellence: give all higher education institutions complete autonomy. Let them all compete and get better. In tandem with increased transparency and accountability on outcomes, all the stakeholders—students, industry, society and nation—will benefit.
Encourage 40-50 philanthropists to establish world-class universities: removing the regulatory hurdles for all at the outset, and letting them earn their eminent status from stakeholders, just like Stanford and all world-class universities have done, is far more effective and equitable.
Create a new agency that provides research funding on merit to faculty members in both public and private universities. This is a well-accepted practice around the world. Peer-reviewed by experts in respective fields, the increased research funding will spur competition between faculty members and institutions, catalyze India’s research and innovation ecosystem, and accelerate solving the nation’s grand challenges.
Conclusion
It is time to unshackle India’s higher education system from the British Raj rules, regulations, and mindset. With a tsunami-scale wave of youth at the gates of higher education, India cannot afford to transform the system six Institutes of Eminence at a time. It is time to make urgent and comprehensive reforms. Now.